Health & Fitness
Medicare Covers Power Wheelchairs For Life At Home. Disabled New Yorkers Need Them For Life Outside It.
After a Medicare fraud crackdown, wheelchair approvals got more complex. A Patch investigation found denied amounts more than tripled.


Editor’s Note: This Patch investigation was reported with support from Investigative Reporters and Editors’ 2025 Koch Continuum Grant, which funds public health and disability reporting.
NEW YORK, NY— In between calls with patients, a Brooklyn psychologist stared at the letter addressed to her from the Centers for Medicare & Medicaid Services.
But Nina Bakoyiannis hesitated to read the words she had waited six months for.
Find out what's happening in New York Cityfor free with the latest updates from Patch.
Because after years of enduring the same process, she knew that etched in formal jargon, and the sort of robotic apathy she would never offer one of her own patients, lay the verdict of her livelihood.
As she sat in a chair with corroded wheels and an aging joystick that moved with the stubbornness of a decades-old arcade game, she read the determination:
Find out what's happening in New York Cityfor free with the latest updates from Patch.
"Not medically necessary."
Bakoyiannis uses a Permobil Corpus power wheelchair with tilt, recline and seat elevation to manage a disability she has had since birth.
The seat elevation function allows her to raise herself to reach countertops, transfer safely and reduce pressure on her body throughout the day.
“Most people don’t think about what an intimate relationship it is to have a wheelchair,” Bakoyiannis said. “This is the thing that holds your body and moves you around the world.”
While her occupational therapist submitted the initial application, she decided to write a letter to Medicare herself: explaining how losing the feature would affect her independence.
A couple months later, when she found herself in the same position, staring at another letter from Medicare, she didn't know what shocked her more— the second denial, or the suggestion to correct it.
In response, she said, Medicare asked her to submit video footage demonstrating how she would use the equipment inside her apartment.
“Is this a reasonable and humane thing to ask someone to record themselves doing tasks like using the bathroom and showering?” Bakoyiannis asked.
She refused. She cited privacy concerns and asked where such a requirement appeared in policy.
Instead, her occupational therapist submitted revised documentation explaining the specific daily activities that required seat elevation. The feature was ultimately approved.
In total, it took about eleven months for Bakoyiannis to receive her power wheelchair with the correct modifications.
“You are literally bedbound and stuck, unless you have access to a backup chair,” she said. “It made me think about how much power these systems have over disabled bodies.”

The Centers for Medicare & Medicaid Services updated its coverage policy in 2023 to recognize power seat elevation as medically necessary for certain users of complex power wheelchairs when clinical criteria are met, including documented needs for reaching and transferring inside the home and evaluation by a specialty team.
Bakoyiannis’ experience was not the result of a single denial or a single insurance reviewer.
It unfolded inside a system that has spent decades trying to balance fraud prevention, cost control and medical necessity, by increasingly sorting power wheelchairs into narrow Medicare categories that require more detailed documentation before approval.
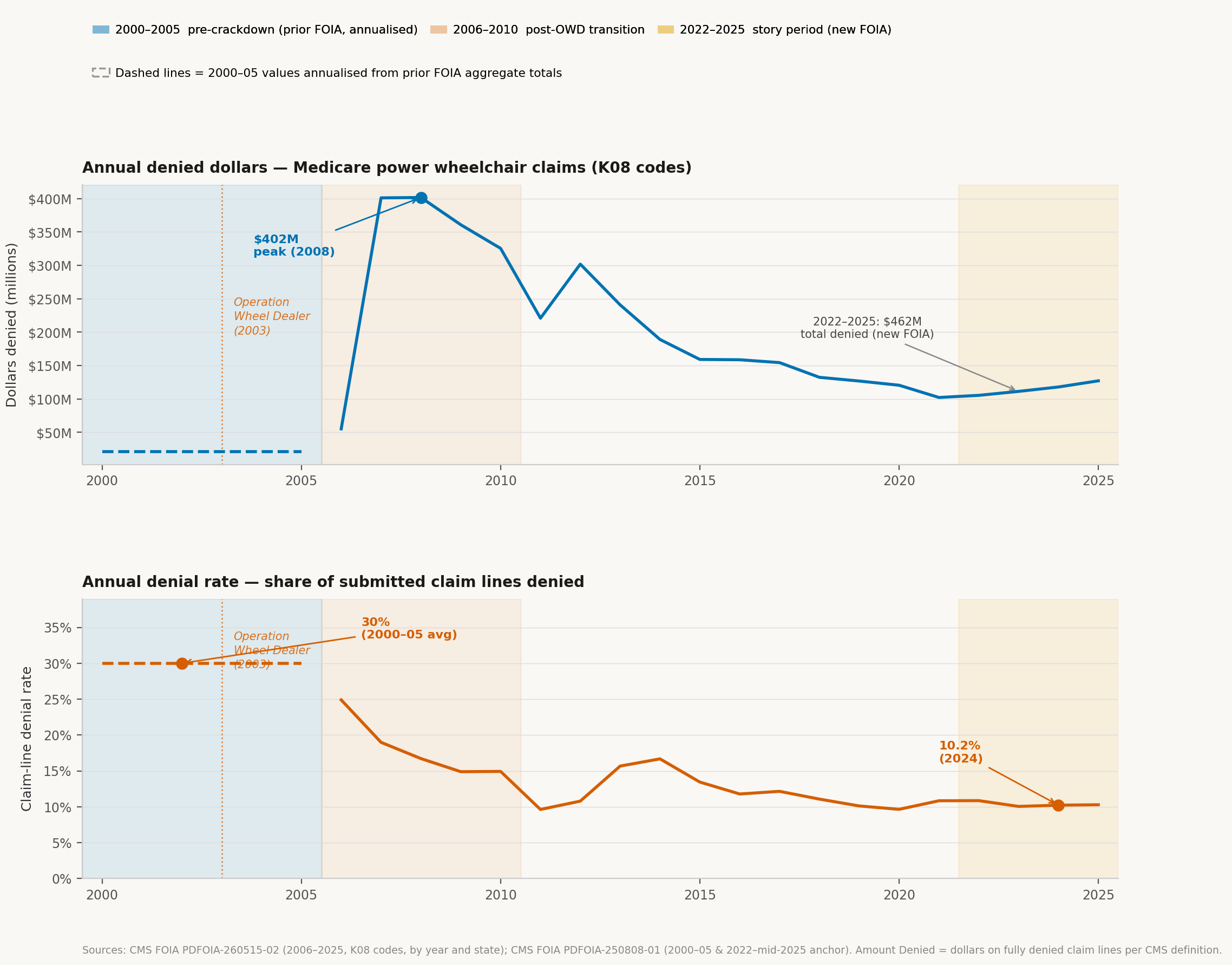
A Patch analysis of CMS data obtained through a Freedom of Information Act request shows a Medicare power-wheelchair system in which denial rates have fallen at the billing-line level, even as the Medicare-valued dollars attached to denials have risen sharply.
The analysis treats a “claim” as a power-wheelchair billing submission at the HCPCS code-line level.
It defines “denied dollars” as the Medicare-allowed amount associated with denied billing lines, not the supplier’s submitted charge or list price.
Because suppliers often bill above Medicare’s reimbursement rates, submitted charges are not equivalent to program payments; the figures reflect Medicare’s standardized valuation of denied claims.
From 2000 through 2005, Medicare processed about 64,469 power-wheelchair billing lines, or roughly 10,745 a year.
From January 2022 through July 2025, that number rose to more than 740,000, or about 208,496 annually.
Over the same span, the denial rate fell from 30 percent to 13.47 percent.
The Medicare-allowed amounts tied to denied claims moved in the opposite direction.
Total denied allowed amounts rose from $126 million in the earlier period to $1.163 billion in the later period.
After adjusting the earlier period for inflation, denied allowed amounts rose from roughly $300 million to just over $1.1 billion — more than tripling even as claim-line denial rates fell.
Editor’s Note: The comparison uses period midpoints (approximately 2002–03 for the early period and 2023–24 for the later period) to account for differences in time span and partial-year reporting in the most recent data. Inflation adjustments primarily affect the earlier period, as most of the price level change occurred over the past two decades, while the later-period values are already near current dollars.
Physical therapist Jean Minkel had been fitting wheelchairs in New York City long before power mobility became a billion-dollar Medicare business.
When she entered the field in 1982, the market for power wheelchairs was, in her words, dust.
There were only a handful of models, and most were bulky rear-wheel-drive machines.
Then, as the 1990s ushered in a wave of technological innovation, the durable medical equipment market changed with it.
Manufacturers introduced new designs. Rear-wheel-drive chairs were joined by mid-wheel-drive models that could turn sharply enough to navigate kitchens, hallways and apartment bathrooms.
Power wheelchairs became more customizable, and seating systems became more sophisticated.
What had once been a relatively uniform category of equipment began to diversify.
At the same time, the industry itself was splitting into two distinct worlds.
One consisted of what clinicians often call consumer power chairs: devices intended for people who could still walk short distances, but lacked the endurance to travel farther.
The other was the population Minkel spent most of her career serving.
Unlike consumer power-chair users, these individuals depend on wheeled mobility as their primary means of movement and require wheelchairs tailored to their bodies, environments and daily routines.
Their chairs addressed far more than transportation. Many users lacked sensation and faced the constant risk of pressure injuries. Others required specialized supports simply to sit upright against gravity.
To view the full map click here:
Then came Harris County, Texas.
In 1998, roughly 3,000 power wheelchairs were sold there. A year later, that figure had climbed to about 30,000.
Investigators later alleged that some physicians and suppliers had learned how to exploit Medicare's paperwork requirements— checking boxes on certificates of medical necessity, billing for expensive equipment and, in some cases, delivering cheaper devices or no equipment at all.
By 2003, federal officials were confronting what they viewed as a crisis.
Medicare spending on power mobility devices had risen from $289 million in 1999 to $1.2 billion in 2003.
The number of reimbursements had nearly tripled, climbing from 55,000 to 159,000.
That March, CMS launched Operation Wheeler Dealer, an anti-fraud initiative conducted with the Department of Justice. The effort ultimately recovered $84 million in fraudulent claims.
Then-CMS Administrator Thomas Scully said that while many wheelchairs were being provided by ethical suppliers to beneficiaries who genuinely needed them, a “great number of unscrupulous suppliers" were promising free wheelchairs to people who did not.
In May 2005, CMS issued a new National Coverage Determination for mobility assistive equipment, including wheelchairs.
The policy tied coverage to whether a beneficiary needed the equipment to perform what Medicare defined as “mobility-related daily activities” inside the home, such as bathing, dressing and using the bathroom.
CMS later added documentation rules requiring more detailed clinical evaluations before mobility equipment could be approved.
In response to a request for comment, Melissa Rumley, a public affairs specialist with the U.S. Department of Health and Human Services Office of Inspector General, said CMS “could better speak to its Operation Wheeler Dealer initiative, its effects, and resulting policies” and declined to comment.
Patch sought comment from CMS, National Seating & Mobility, NuMotion and manufacturers named in this story. CMS did not respond to multiple requests for comment.
The CMS policy change resulted in more strenuous application requirements and longer approval times, Minkel said.
But, most importantly, it narrowed a wheelchair’s purpose for users: life inside the home, rather than beyond it.
Before the policy shift, clinicians considered whether a chair would allow someone to work, go to school, use public transportation and participate in community life.
In practice, Minkel could recommend a power wheelchair that met a person’s needs across all of their daily environments, she said.
Now, she said, what once centered on a person’s full lifestyle has been reduced to what they can do at home.
For wheelchair users in New York City, it can determine whether someone receives equipment built for the sidewalks and streets they navigate every day, Minkel said.
She described patients who can move short distances inside a small apartment using a cane or walker, but cannot travel independently beyond it.
“If you put them outside the front door,” Minkel said. “They can’t make it up the block to go get the bus.”
Minkel, now senior vice president of care coordination and rehabilitation services at Independence Care System, said her nonprofit helps people with significant disabilities navigate New York and maintain independence.
“We called them our urban cowboys,” Minkel said. “They were constantly moving through the City.”
The nickname referred to people who relied on their chairs to travel every day: navigating cracked sidewalks, curb cuts, subway stations and buses.
Minkel said her organization tried to preserve old chairs as backups because mobility loss could disrupt a person’s entire life.
“It wasn’t a question of whether their primary chair would break down,” she said. “It was when.”
She pointed to a broader shift in how wheelchairs are categorized and covered under Medicare.
According to data analyzed by Patch, power-wheelchair billing was once concentrated in just four main Medicare categories.
Over time, that system expanded to 59, becoming far more detailed and requiring more documentation to justify each feature and function.
Within that structure, Minkel drew a distinction between Group 3 and Group 4 power wheelchairs.
Group 3 chairs are complex rehabilitation devices for people with significant mobility impairments.
Group 4 chairs are built for higher performance, with stronger motors and more durable frames—equipment better suited for heavy, continuous use in environments like New York City, she said.
Medicare generally does not cover Group 4 capabilities, treating them as unnecessary for use inside the home.
“If you’re living in New York City, and you’re going up and down curb cuts and trying to get on and off public transportation, the Medicare-approved power wheelchairs just weren’t built for that,” Minkel said.
In practice, Group 3 represents the most advanced level of wheelchair typically reimbursed under Medicare, she said.
Because the code systems are not directly equivalent across eras, Patch analyzed aggregate totals rather than comparing individual codes one by one.
That distinction shows up in the data through one billing code: K0861, a Group 3 power wheelchair code covering complex devices with multiple powered functions.
That code accounted for $462 million in denied allowed amounts between 2022 and July 2025, according to CMS data.
Nearly 40 percent of all denied allowed amounts in the analysis came from that code.
On average, denied billing lines under K0861 carried a Medicare-allowed amount exceeding $47,000.
To view the full chart click here:
The federal data does not show why individual claims were denied, whether appeals succeeded, whether beneficiaries eventually received equipment after delays, or whether they obtained wheelchairs through Medicaid, private insurance or private fundraising.
In New York, providers submitted 23,161 power-wheelchair billing lines from 2022 through July 2025.
Medicare denied 2,701 of them, a denial rate of 11.7 percent.
Those denied lines represented $5.4 million in denied allowed amounts.
Separately, providers’ submitted charges exceeded Medicare-allowed amounts by $48.5 million, a measure of the gap between supplier billing and Medicare valuation, not the amount Medicare would have paid.
The result, Minkel said, is a system that reimburses wheelchairs for one kind of use, while people rely on them for another.
That is the argument at the center of a discrimination complaint brought by Disability Rights Education and Defense Fund attorneys on behalf of Saleema Render Hornsby, a young New York City wheelchair user with spina bifida.
The complaint alleges that CMS’ in-home use policy violates Section 504 of the Rehabilitation Act by unnecessarily segregating disabled people from community life.
It argues that Medicare law does not require coverage to be limited to activities inside the home, but that CMS has adopted an interpretation that effectively denies equipment needed for participation outside it.
According to the complaint, Hornsby uses a walker for short distances inside her home, but relies on a wheelchair for travel outside it.
With an appropriate chair, she is able to go to the gym, attend cosmetology school, shop for groceries, pick up prescriptions and get to medical appointments.
Between 2019 and 2022, her previous power wheelchair broke down at least five times while she was in the community.
Once it stopped in the middle of a busy intersection, leaving her stranded in the street. Another time, it failed on a beach ramp, where she had to rely on strangers for help.
In 2022, a mobility clinic recommended an ultralight manual wheelchair with a power assist feature.
Medicare denied the request, saying the documentation did not demonstrate that the device would improve her ability to perform mobility-related activities of daily living or that it would be used consistently inside the home.
Her Medicaid managed care plan also denied coverage.
After appeals and additional review, she received the chair on October 27, 2023— more than a year and a half after it was first recommended.
During that time, she missed medical and dental appointments, stopped going to the gym, and was unable to pick up prescriptions or grocery shop consistently.
She also withdrew from in-person cosmetology training after switching to online classes.
The disruption, the complaint states, contributed to depression, and she began seeing a therapist.
Silvia Yee, a senior attorney at Disability Rights Education & Defense Fund who helped file the complaint, said it has received little response from the Department of Health and Human Services’ Office for Civil Rights since it was submitted.
She said that while such filings typically receive at least an acknowledgment, no meaningful update has followed more than a year later.
“Those policies over 20 years have had these unforeseen and unwanted consequences,” Yee said. “Someone’s writing this who doesn’t really know why people use wheelchairs.”
Hornsby’s experience was not unusual, according to a 2025 survey of 143 Medicare mobility-device users.
The survey found that 63 percent of respondents said obtaining a wheelchair was difficult or very difficult.
In the past five years, 41 percent had been denied coverage for a wheelchair or wheelchair component, and nearly one-third said their final device did not meet their needs at home or in the community.
Nearly a quarter of recent wheelchair purchases in the survey were not covered by medical insurance.
In practice, that often meant people turning to private funding.

Savannah Grayson, who has cerebral palsy, has long been into fashion, treating clothing and styling as a form of self-expression as much as personal routine.
Born and raised in Queens, when the Knicks won the championship on Saturday, she celebrated in a full, coordinated outfit, dressed head-to-toe in orange and blue.
Because she can take a few steps inside her home, she said she has not qualified for Medicare coverage for mobility equipment under existing eligibility rules, even though she relies on a wheelchair to move through the City.
Instead, she has relied on GoFundMe campaigns, friends and informal networks.
Her fundraisers, she said, usually meet their goals within a week or less—faster, she noted, than the insurance process itself.
This year, the 26 year old moved into her own one-bedroom apartment in Rockaway Beach—an achievement she describes as a major marker of independence.
“But not everyone has the community or resources to raise money for a wheelchair,” Grayson said.
In the decades before the disability rights and deinstitutionalization movements gained momentum, hundreds of thousands of Americans with disabilities lived in large institutions.
More than 200,000 people with intellectual and developmental disabilities were still living in institutions as late as 1977.
Mary Lou Breslin, a wheelchair user and co-author of the Disability Rights Education & Defense Fund survey, said Medicare’s “in the home” language, written in 1964, reflected a shift toward recognizing disabled people as community members rather than institutional residents.
“It was extremely progressive for the phrase to be in the regulations,” Breslin said. “But it’s kind of weird how it got completely twisted into the interpretation that we’re living with.”
Breslin said the policy shift did not just change approvals. It changed what manufacturers chose to build.
She described a power wheelchair she had relied on for years as durable, compact and reliable.
It could travel roughly 27 miles on a charge, she said, and withstand heavy daily use.
Airlines, she said, struggled to damage it during transport.
Then, slowly, the model disappeared.
Breslin said the chair no longer fit the coding and reimbursement structure that took shape after Medicare’s policy changes.
Once the relevant billing code was removed, she said, the chair was no longer financially viable to produce.
Now, she and other users try to keep aging versions of the chair alive with spare parts.
“It’s like I’m the Montana survivalist in my garage,” Breslin said.
As reimbursement categories narrowed and cost pressures intensified, she said, manufacturers began building around what Medicare would cover: prioritizing lower-cost production and coding compatibility over durability and long-term performance.
According to data analyzed by Patch, the number of suppliers billing Medicare for power-wheelchair equipment dropped from 5,552 to 1,912 between the two periods— a decline of about 66 percent.
But the remaining companies processed far more claims, consolidating the system into fewer hands.
Minkel said New York City once had several smaller complex rehabilitation providers.
By 2019, she said, much of the local market had consolidated around two national companies: National Seating & Mobility and NuMotion.
NuMotion and National Seating & Mobility did not respond to requests for comment about their roles in Medicare power-wheelchair provision and repair services.
“What they did was they went around and they purchased all of these little complex rehab companies,” Minkel said.
She said the effects were visible in repairs.
Smaller providers once maintained long relationships with users and technicians.
A wheelchair user might call a technician they knew by name, ask for batteries and get routine issues addressed quickly.
“Very few people have that now,” she said.
For Minkel, consolidation, reimbursement pressure and repair delays are now linked.
“We have an industry with very little innovation when it comes to improved technology,” she said. “And you wonder why there’s repair problems.”
At least one manufacturer said reimbursement pressure has affected what companies can afford to build and support.
R.D. Davidson, chief operating officer of 21st Century Scientific, Inc., which manufactures the BOUNDER power wheelchair, said durable chairs require stronger frames, reliable electronics, quality motors, testing, replacement parts, and technical support, all of which increase cost.
“When reimbursement is too low, the industry is pushed toward cost containment instead of long-term value,” Davidson said in a written response to Patch. “This results in vendors supplying lower cost, less durable products that fit the funding allowables.”
He added that dense urban environments place heavy stress on power wheelchairs, increasing vibration and impact that accelerates wear on batteries, tires and upholstery.
New York’s 2023 “right-to-repair” law was designed to loosen manufacturers’ control over how electronic devices are serviced once they are sold in the state.
It requires covered manufacturers to provide access to diagnostic tools, parts, and technical documentation that match what is available to authorized repair networks.
But medical devices, including power wheelchairs, are explicitly excluded from its protections.
That exclusion means wheelchair users remain dependent on the existing supplier, insurer and manufacturer repair pipeline.
Once technicians arrive, scheduling constraints and travel requirements extend turnaround times further, especially in dense urban environments like New York City.
When Breslin needed replacement armrest pads, she bypassed the repair pipeline entirely, ordering parts online for about $10 and installing them herself.
A 2016 study of 591 wheelchair users with spinal cord injuries found that breakdowns were common and often disabling.
Nearly two-thirds reported needing at least one repair within a six-month period.
Among those, more than a quarter experienced serious consequences tied to the delay or failure to repair—most often being stranded without mobility.
In the most severe cases, 18.2 percent said they were left entirely stranded.
State-level oversight reviews show a similar pattern.
A Connecticut Wheelchair Repair Task Force, drawing on an informal survey of 73 users, found that 56 respondents waited at least a month for repairs, with many reporting delays stretching beyond six months.
The task force also documented how the repair pipeline itself contributes to those timelines: in-home assessments averaged 24 to 27 days, compared with just two to four days for evaluations conducted remotely or in a shop.
Once replacement parts arrived, installation in the home typically required another 25 to 27 days— effectively adding months to even routine fixes.
By November 2023, the task force reported substantial service backlogs among major suppliers.
NuMotion had 740 open service orders affecting 622 customers, while National Seating & Mobility reported 687 orders across 445 customers.
Industry representatives attributed delays to a combination of constrained parts supply chains, prior authorization requirements, staffing shortages, transportation challenges, and the time required to conduct in-home service visits.
At the same time, providers told the task force that the structure of the system itself limits capacity: most assessments are conducted in users’ homes rather than in centralized facilities, extending travel and turnaround times for technicians.
The task force ultimately did not reach consensus on remedies.
Disability advocates urged enforceable timelines requiring in-home assessments and repairs within four business days, or six calendar days after all external steps were completed.
Industry representatives opposed statutory deadlines, arguing that repair timelines depend on variables such as parts availability, authorization processes and field logistics that cannot be uniformly controlled.
While Bakoyiannis could not fathom the idea of proving need by attempting to shower or cook without proper equipment, the timeline itself never surprised her.
A new chair, she said, takes about a year. Repairs take a couple of months.
Bakoyiannis said she typically needs repairs at least once a year, a rhythm shaped by New York City living, where batteries drain under constant use, wheels wear down on uneven sidewalks, casters rust after rain and snow, joysticks begin to fail from daily strain, and footplates eventually break.
When something fails, she said, the long process begins again. A technician first evaluates the chair. Documentation is sent to her physician. The physician signs forms. The supplier submits paperwork to the insurer. The insurer decides whether the repair is covered. Only then can parts be ordered and work scheduled.
At 31, Bakoyiannis had built her life around the promise of her profession.
Sitting in her waterfront Williamsburg apartment, she seems to embody what many native New Yorkers strive for: a life built entirely in the city that raised them.
She earned her PhD in Clinical Psychology from Long Island University in Brooklyn and built her early career in its hospitals, clinics and classrooms.
Now a clinical psychologist, she works full time in private practice while continuing postdoctoral clinical work.
She also teaches as an adjunct assistant professor of undergraduate psychology at Brooklyn College, moving between patients, students and supervision across the same boroughs she has long called home.
Still, she said, the repair process is often dictated by technicians’ schedules, leaving wheelchair users to adjust their lives around when appointments are available.
“A lot of disabled people work,” Bakoyiannis said. “I can’t just be home all day waiting for someone to maybe show up.”
She described repeated difficulty getting responses from National Seating & Mobility.
She said she left messages that were not returned and had to call repeatedly to follow up on repair requests.
In one case, she completed a video evaluation for a footplate issue and was told someone would contact her. No one did, she said.
Eventually, she scheduled an in-person appointment herself.
“I don’t think that it’s anyone’s individual fault,” she said. “I think there’s just not enough people that work there.”
In five years, Bakoyiannis will go through the process again: submitting documentation meant to prove what her body already knows.
And then, once the chair is finally approved, the slow return of the same maintenance cycle she is already living through now.
By then, the system will not feel more flexible than it does today, she said.
It will only feel familiar.
“You really have to hold these two systems’ hands,” Bakoyiannis said. “And make sure they’re actually communicating to each other.”
Get more local news delivered straight to your inbox. Sign up for free Patch newsletters and alerts.


